Description
3rd generation weight management peptide
Retatrutide 10 mg is a research-grade triple agonist peptide supplied in lyophilised form for laboratory use. It acts on GLP-1, GIP and glucagon receptors and has attracted strong interest in metabolic research, particularly in models of appetite regulation, body-weight change, glycaemic control and energy balance.
Retatrutide belongs to a newer class of investigational metabolic peptides designed to engage multiple receptor pathways simultaneously, rather than targeting GLP-1 alone. This makes it especially relevant in research focused on incretin biology, glucose homeostasis, energy expenditure and next-generation obesity models. Because of its broad receptor activity, Retatrutide is considered a step beyond traditional GLP-1 analogues, offering a new horizon for studies in obesity and related conditions. Compared to dual agonists such as Tirzepatide and single-pathway compounds like Semaglutide, Retatrutide represents a broader multi-pathway research model. For a detailed comparison of incretin-based compounds, see our GLP-1 metabolic research guide.
What is Retatrutide?
Retatrutide is an investigational triple agonist peptide developed to activate three key receptor systems involved in metabolic regulation:
- GLP-1 receptor
- GIP receptor
- glucagon receptor
This receptor profile makes Retatrutide mechanistically broader than Semaglutide and Tirzepatide. Semaglutide primarily targets GLP-1, while Tirzepatide combines GLP-1 and GIP activity. Retatrutide adds a third component — glucagon receptor agonism — which is one of the reasons it has drawn so much attention in metabolic and obesity-related research. Retatrutide is described in the literature as an investigational triple-hormone receptor agonist with activity across all three pathways.
Why Retatrutide matters in metabolic research
Retatrutide is being studied because it combines incretin signalling with glucagon-receptor activity, creating a broader metabolic profile than standard GLP-1 analogues.
In the literature, Retatrutide has been investigated in relation to:
- body-weight regulation and appetite signalling
- glucose metabolism and glycaemic markers
- energy expenditure and substrate utilisation
- multi-pathway incretin research
- next-generation obesity and metabolic-disease models
For researchers comparing newer metabolic peptides, Retatrutide is often discussed alongside Semaglutide and Tirzepatide because it extends beyond GLP-1/GIP into triple-pathway metabolic modulation. Reviews and overviews consistently describe it as a multi-receptor peptide being studied for obesity and metabolic control, with a receptor profile broader than earlier incretin agents.
How Retatrutide works
Retatrutide is designed to activate three receptor systems involved in metabolic control:
GLP-1 receptor activity
GLP-1 signalling is associated with appetite reduction, delayed gastric emptying and glucose-dependent insulin support. This is the pathway most researchers already know from compounds such as Semaglutide.
GIP receptor activity
GIP signalling is thought to influence insulin secretion, nutrient handling and adipose metabolism. In dual-agonist and triple-agonist research, it may contribute to a broader incretin response than GLP-1 alone.
Glucagon receptor activity
This is the major differentiator. Glucagon-receptor activation is being studied for its role in energy expenditure, hepatic metabolism and body-weight regulation, making Retatrutide mechanistically broader than both Semaglutide and Tirzepatide.
Together, these pathways make Retatrutide a useful model compound for research into multi-receptor metabolic signalling rather than single-pathway incretin activity alone. Eli Lilly’s own overview and recent review literature both describe Retatrutide as a once-weekly investigational triple agonist acting on GLP-1, GIP and glucagon receptors.
Published clinical findings on Retatrutide
Retatrutide has attracted unusual attention because human clinical studies have reported substantial effects on body weight, glycaemic markers and broader cardiometabolic parameters. In published phase 2 research in adults with obesity or overweight, investigational retatrutide produced dose-dependent weight reduction, with the highest-dose groups showing some of the strongest body-weight outcomes reported so far for an incretin-based agent.
More recently, Eli Lilly reported phase 3 obesity data from TRIUMPH-1, where participants on the 12 mg arm lost an average of 28.3% of body weight over 80 weeks, with a substantial share achieving at least 30% weight loss. Those results are not yet the same as an approved product label, but they materially strengthen Retatrutide’s position as one of the most closely watched next-generation metabolic peptides in development.
Retatrutide has also shown clinically meaningful effects in type 2 diabetes research. In Lilly’s phase 3 TRANSCEND-T2D-1 results, Retatrutide reduced HbA1c by roughly 1.7% to 2.0%, alongside substantial weight loss, reinforcing the idea that its triple-agonist profile may extend beyond appetite and body weight into broader metabolic control.
Published safety and tolerability findings
Published clinical studies on investigational Retatrutide indicate that the most commonly reported adverse events are gastrointestinal, especially nausea, diarrhoea, vomiting and constipation. In the phase 2 obesity trial published in the New England Journal of Medicine, these events occurred more often with Retatrutide than with placebo, were generally dose-related, and were reported predominantly during the dose-escalation period. Most were described as mild to moderate in severity.
The phase 2 data also suggest that tolerability may be influenced by the starting dose and escalation schedule. Gastrointestinal adverse events were partly mitigated when escalation began from 2 mg rather than 4 mg, which is consistent with the broader incretin-drug class, where tolerability often improves with slower titration. Dose-dependent increases in heart rate were also reported, peaking during the trial and declining later.
As with other incretin-based agents, adverse events were one of the main reasons for treatment discontinuation in clinical trials, especially at higher doses. For that reason, Retatrutide’s clinical profile is usually discussed not only in terms of weight-loss efficacy, but also in terms of tolerability during escalation, GI event burden, and the balance between efficacy and dropout risk. This section summarises published findings on investigational Retatrutide, not instructions or expectations for use of this product.
Published dosing schedules used in Retatrutide research
Published clinical studies on investigational Retatrutide used once-weekly subcutaneous administration with stepwise dose escalation rather than fixed full-dose initiation. In the phase 2 obesity trial published in the New England Journal of Medicine, participants were assigned to several dose arms: 1 mg, 4 mg, 8 mg and 12 mg, with some higher-dose groups starting at a lower introductory dose before escalating. Specifically, the trial included 4 mg with an initial dose of 2 mg, 4 mg with an initial dose of 4 mg, 8 mg with an initial dose of 2 mg, 8 mg with an initial dose of 4 mg, and 12 mg with an initial dose of 2 mg, all administered once weekly for 48 weeks.
In practical terms, that means published Retatrutide research did not use a single universal schedule. The phase 2 program tested both slower escalation and faster escalation approaches to reach the same maintenance dose, which is one reason the study is useful not only for efficacy, but also for tolerability comparisons. For example, some 8 mg groups began at 2 mg and escalated upward, while others began at 4 mg before reaching the same target dose. The 12 mg arm also used 2 mg as the initial dose before escalation.
The type 2 diabetes phase 2 study used a similar logic. Participants received once-weekly Retatrutide at 0.5 mg, 4 mg, 8 mg, or 12 mg, with separate escalation and non-escalation arms in some groups — again highlighting that the published research focused heavily on dose-escalation strategy, not only on final dose.
| Published study arm | Initial dose used in the trial | Target dose | Frequency | Study duration |
|---|---|---|---|---|
| Obesity phase 2 | 1 mg | 1 mg | once weekly | 48 weeks |
| Obesity phase 2 | 2 mg | 4 mg | once weekly | 48 weeks |
| Obesity phase 2 | 4 mg | 4 mg | once weekly | 48 weeks |
| Obesity phase 2 | 2 mg | 8 mg | once weekly | 48 weeks |
| Obesity phase 2 | 4 mg | 8 mg | once weekly | 48 weeks |
| Obesity phase 2 | 2 mg | 12 mg | once weekly | 48 weeks |
These schedules are included as a summary of published research design and are not instructions for use of this product.
Retatrutide vs Semaglutide vs Tirzepatide
Researchers often compare these compounds because they sit on the same metabolic spectrum, but they are not interchangeable.
Retatrutide
- Triple agonist: GLP-1 + GIP + glucagon
- Broadest receptor profile of the three
- Often discussed in relation to body-weight outcomes, appetite regulation and energy expenditure
- Dual agonist: GLP-1 + GIP
- Positioned between Semaglutide and Retatrutide in mechanism
- Widely studied for glycaemic control and body-weight effects
- Single agonist: GLP-1
- Best-known and most established of the three
- Common reference point for GLP-1 pathway research
For researchers building a metabolic peptide panel, Retatrutide is generally the most relevant when the goal is to explore triple-pathway signalling rather than standard GLP-1 activity alone.
Product characteristics
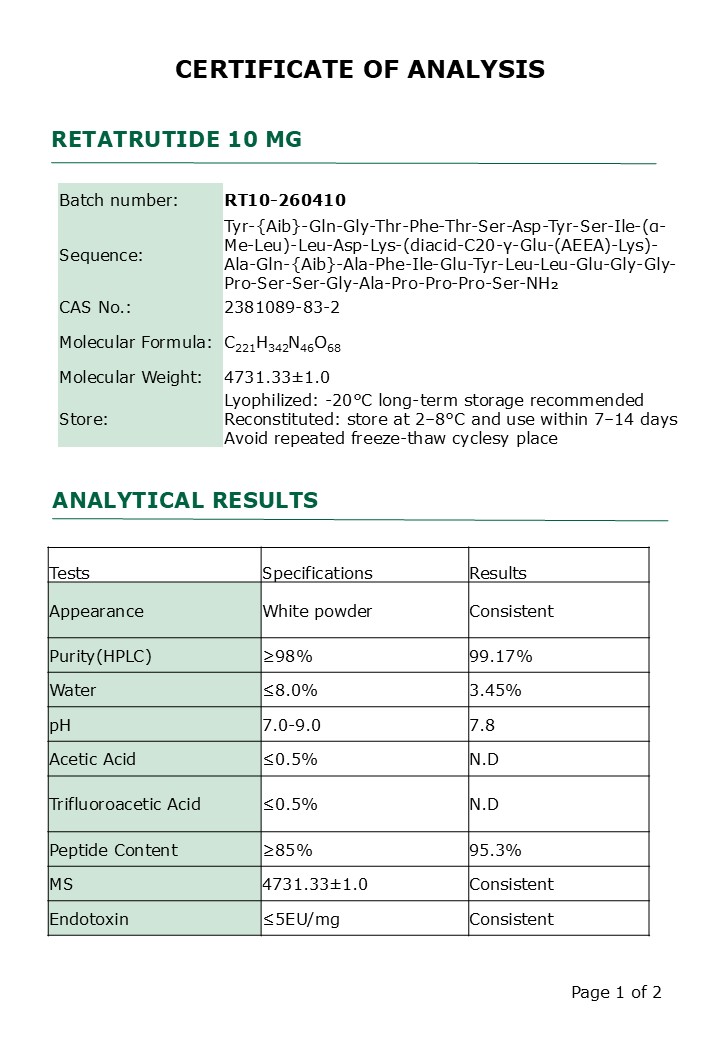
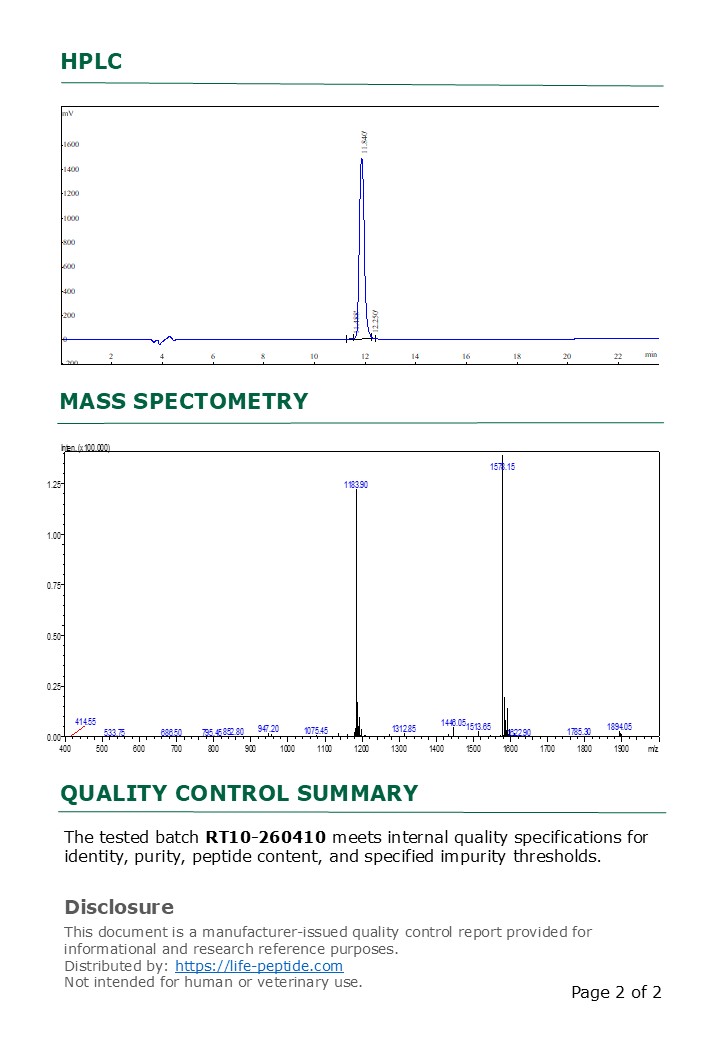
Purity: ≥ 99% (HPLC) with batch-specific COA
Appearance: white lyophilized powder
Molecular formula: C221H342N46O68
Molecular weight: 4731.33±1.0
Sequence: Tyr-{Aib}-Gln-Gly-Thr-Phe-Thr-Ser-Asp-Tyr-Ser-Ile-(α-Me-Leu)-Leu-Asp-Lys-(diacid-C20-γ-Glu-(AEEA)-Lys)-Ala-Gln-{Aib}-Ala-Phe-Ile-Glu-Tyr-Leu-Leu-Glu-Gly-Gly-Pro-Ser-Ser-Gly-Ala-Pro-Pro-Pro-Ser-NH₂
Produced in GMP-compliant facilities under strict QC protocols.
Each batch carefully lab tested after production (you can find Certificate of Analysis under product pictures).
Freeze-dried (lyophilized) for maximum stability and extended shelf life.
Sealed in sterile vials, ready for reconstitution.
Application: laboratory and analytical research
Storage: unopened lyophilized vials are best stored refrigerated at 2–8°C, which is the storage method confirmed by our manufacturing partner and suitable for up to 24 months. Refrigeration is preferred because it minimizes unnecessary freeze–thaw cycles during routine handling. If substantially longer-term storage is required, unopened lyophilized vials may also be kept frozen. Once reconstituted, always store at 2–8°C and do not freeze.
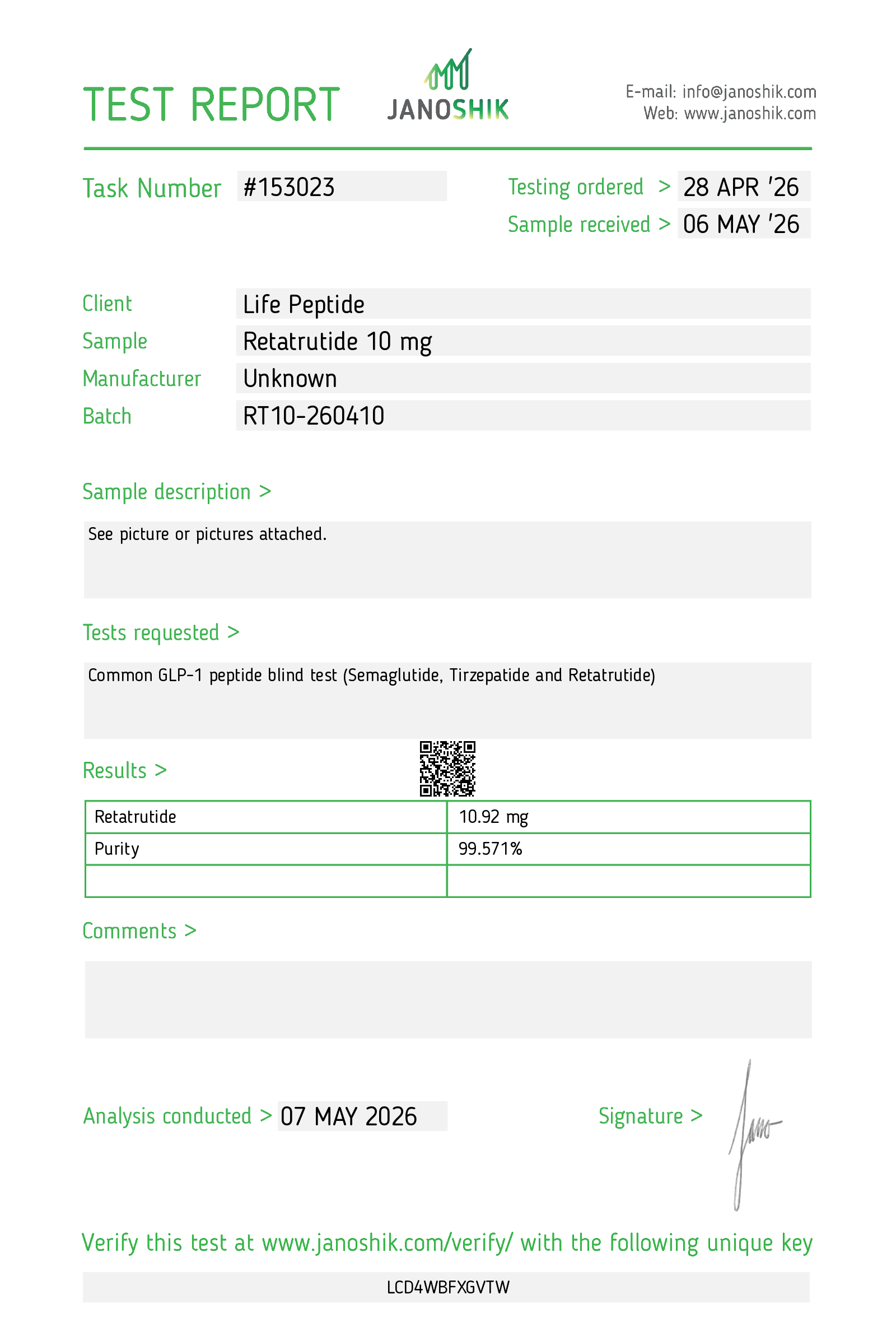
Independent third-party verification
This batch has undergone additional third-party analytical verification through Janoshik Analytical
Batch: RT10-260410
Internal HPLC purity: 99.17%
Third-party verification: 99.57% independently confirmed high purity and identity consistency. View third-party verification.
Reconstitution and handling
Retatrutide is supplied as a lyophilised vial and should be handled using standard peptide reconstitution procedures appropriate to the research setting. It must be reconstituted with bacteriostatic water before use. GLP-1 class peptides are sometimes slow to dissolve and require very gentle reconstitution to avoid foaming or remaining slightly cloudy.
For other solvent selection, concentration planning and storage guidance, see the full Peptide Reconstitution Guide and Reconstitution Calculator
Selected research references
- Jastreboff AM et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity. New England Journal of Medicine, 2023.
- Coskun T et al. LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss: from discovery to clinical proof of concept. Cell Metabolism, 2022.
- Katsi V et al. Retatrutide—A Game Changer in Obesity Pharmacotherapy. 2025 review article.
FAQ
What kind of peptide is Retatrutide?
Retatrutide is an investigational triple agonist peptide designed to activate GLP-1, GIP and glucagon receptors.
How is Retatrutide different from Semaglutide?
Semaglutide targets GLP-1 only, while Retatrutide combines GLP-1, GIP and glucagon receptor activity, giving it a broader metabolic signalling profile.
How is Retatrutide different from Tirzepatide?
Tirzepatide is a dual GLP-1/GIP agonist. Retatrutide adds glucagon receptor activity, which is one of the main reasons it has attracted attention in next-generation metabolic research.
What research areas is Retatrutide associated with?
Retatrutide has been studied in the literature in relation to body-weight outcomes, appetite regulation, glycaemic control, incretin signalling and energy metabolism.
Is this product intended for human use?
No. This product is supplied strictly for research use only and is not intended for human consumption or therapeutic use.
Related research context
Retatrutide is part of the GLP-1/GIP/glucagon triple-receptor agonist metabolic research class. For mechanistic comparison with single and dual agonists, see our GLP-1 metabolic research guide.
Browse all compounds in the Metabolic research category.
Researchers comparing multi-receptor activation may also examine:
- Tirzepatide (GLP-1/GIP dual agonist)
- Semaglutide (GLP-1 receptor agonist)
- Cagrilintide
- Blend Cagrilintide + Retatrutide
- Blend Cagrilintide + Tirzepatide
NOTE: This is for educational reference only and does not constitute medical advice.
Disclaimer
This product is sold for research purposes only. It is not intended to diagnose, treat, cure, or prevent any disease. Buyer assumes full responsibility for proper handling and use.
Reviews
There are no reviews yet.